Utilizing Pharmacists and Educational Services to Promote Proper Use of Opioids Across South Carolina
By

By
Kayce M. Shealy, PharmD, BCPS, BCACP, CDE[1]*
Erika E. Tillery, PharmD, BCPP, BCGP[2]**
Cheryl A. Anderson, BS, RPh[3]***
Katelyn L. Cheek, MHA[4]****
Deaths related to opioid overdoses—including prescription and illicit drugs—rose an average of ten to twenty percent per year from 2014 to 2016 in the state of South Carolina (“the State”).[5] In 2015 alone, the number of deaths due to opioid overdose surpassed the overall number of homicides in the State.[6] Additionally, there was a significant increase of sixty-seven percent in the overall number of opioid reversal attempts—through the use of naloxone or another method— made by emergency responders from 2013 to 2016.[7] Due to the escalating crisis, the Governor’s office in South Carolina convened a multi-disciplinary Prescription Drug Abuse Prevention Council and tasked this group to develop an action plan—which was released in December 2014—to combat prescription drug abuse and prevent deaths related to abuse in the State.[8]
The Governor’s Prescription Drug Abuse Prevention Council included more than fifty recommendations in the State Plan to Prevent and Treat Prescription Drug Abuse (Plan) to reduce opioid abuse, misuse, and diversion.[9] The South Carolina Pharmacy Association (SCPhA)—along with the South Carolina Pharmacy Foundation (SCPF)—was awarded a $500,000 two-year grant from the South Carolina Blue Cross Blue Shield Foundation to target specific recommendations proposed by the Plan by developing the preSCriptions Medication Safety Matters project (Project).[10] The SCPhA identified the distinct need to further inform and educate healthcare professionals on prescribing opioids, as well as address dependency and substance use disorders flowing from the use of such medications.[11] The Project also met the critical need to inform and educate South Carolinians of this public health issue and provided suggestions to reduce risk and to receive help.[12] An additional component of the Project was designed to advocate for policy alignment that incentivizes consistent medication prescribing and allows for equitable access to—and consistent payment for—treatment for substance use disorder.[13] Specific goals of the grant included: (1) Increase enrollment in the South Carolina Reporting & Identification Prescription Tracking System (SCRIPTS), the State’s Prescription Monitoring Program; (2) Increase enrollment in opioid treatment programs and substance use disorder treatment; (3) Establish and increase use of safe and approved drug collection disposal programs by establishing at least one site per county; and (4) Decrease deaths related to opioid use.[14]
A goal to decrease incarceration rates related to the violation of laws prohibiting the production, distribution, or use of controlled substances was dropped soon after the start of the project due to an inability to track and record arrests in a comprehensive manner. This Article seeks to provide an overview of steps taken by stakeholders and their respective impact in combatting the opioid epidemic in the State.
At the start of the grant funding period, multi-disciplinary teams were convened to conduct the work of the grant. Teams included a clinical advisory team, an academic detailing team, a clinical data team, and a social media and marketing team.
The Clinical Advisory Team guided the development of—and approved—the toolkit used by the Academic Detailing Team for sessions with providers.[15] This toolkit was based on best practices for chronic pain patients and potential high-risk patients. The Clinical Advisory Team consisted of academic experts, clinicians from the Carolinas Center for Medical Excellence (CCME), professionals from the South Carolina Department of Health and Environmental Control (DHEC), the South Carolina Department of Alcohol and Other Drug Abuse Services (DAODAS), and the SCPhA.
The Clinical Data Team consisted of specialists from DHEC, DAODAS and the South Carolina Office for Healthcare Workforce who provided raw data used to track progress being made in the grant. Data on the number of opioid prescriptions filled prior to the grant’s start in April 2016—and after the completion of the grant in early 2018—was gathered. Data regarding buprenorphine prescriptions dispensed monthly was collected.
The Social Media and Marketing Team utilized the expertise of a local marketing company—with input from the funders of the grant—to develop radio announcements, social media pages and advertisements, and video and print materials targeted toward specific demographic groups within a widely diverse public.
Services included an academic detailing program for provider education and a public awareness campaign for community education that included medication disposal systems. The following section describes each of these services.
Academic detailing is an educational outreach program for clinicians.[16] It provides accurate, up-to-date and relevant drug information in an interactive and one-on-one approach.[17] Clinically trained academic detailers meet with providers in their practice setting to educate them about evidence-based programs.[18]
The Project team contracted Alosa Health—a national organization focused on developing and implementing academic detailing programs to improve prescribing in various clinical areas[19]—to train state-registered pharmacists to perform academic detailing services. The role of academic detailers was to: promote a change in prescribing practices to limit the supply of prescription opioids in circulation; raise awareness of the risk of opioid addiction; help properly identify and treat opioid-dependent patients; and, encourage collaboration with other community initiatives.[20] The Academic Detailing Team prioritized which prescribers received educational visits based on need, prescribing practices, and geographic region. An academic detailing visit could also be initiated by a provider request. High priority was given to areas with high controlled substance dispensing rates and areas of potential abuse, as identified by the State’s drug control agency.[21] Detailing was tailored to individual practices with unique issues and barriers to healthcare.
Alosa Health—with guidance from the Clinical Advisory Team—produced an academic tool for the Academic Detailing Team to utilize when meeting with healthcare providers.[22] The academic tool included the following four areas: (1) A functional approach to chronic pain management; (2) SCRIPTS enrollment and use; (3) Responsible opioid prescribing; and (4) Tapering patients off opioids.[23] At the initial detailing visit, each provider was asked if they were an enrollee and active user of the SCRIPTS program. If they were not, a detailing session would then be focused on enrolling the provider or their delegate(s) and demonstrating the appropriate use of SCRIPTS. The data in SCRIPTS—including the name, strength, dose, quantity, prescriber, dispenser, and date dispensed of the controlled prescription drugs[24]—was reviewed with prescribers. If providers were enrolled and actively utilizing the SCRIPTS program, the visit would focus on chronic pain management—including opioid prescribing and tapering recommendations.
Providing education to the community and raising awareness of the opioid and substance use crisis was a key goal for this Project.[25] Since misuse by family and friends is one of the most common ways that medications—particularly pain relievers—are obtained,[26] the Project focused on medicine cabinets at home. Messaging for the public focused on the dangers of prescription drug misuse and the importance of reducing this risk by keeping prescriptions in a locked or safe place in the home and properly disposing any expired or unwanted medications.[27] Public messaging also sought to destigmatize treatment for substance use disorder and guide individuals to intervention and treatment services. This message coincided with communications to third party payers, promoting safe prescribing practices and equitable access to treatment for substance use disorder to reduce costs and improve population health.
The Project developed a multimedia marketing approach based on heavy use of television, radio, and print advertisements. Advertisements provided statistics on prescription medication misuse in the State and encouraged proper storage and disposal of all medications,[28] particularly those with high risk of misuse (i.e. opioids). Radio announcements were run during peak commuting hours—typically between six am and nine am and between three pm and six pm—on stations across the State and targeted people over the age of forty who would likely have a youth at home.[29] Flyers with information regarding proper storage and disposal of medications—as well as how to recognize a medication overdose—were developed and given to pharmacies throughout the State for distribution to the public.
A website, What’s In Your Cabinet?, was developed as part of the Project to disseminate education.[30] Sections on the website target providers, youth, and caretakers.[31] The “Provider” portal offers resources similar to those highlighted in the Academic Detailing sessions, including prescribing tools for opioids and information related to naloxone.[32] The “Youth” portal connects to Generation Rx, a public initiative with The Ohio State University College of Pharmacy and Cardinal Health Foundation.[33] The “Caretaker” portal provides resources such as a map of treatment facilities for substance use disorder, a map of medication drop box locations across the State, and information about obtaining and using naloxone.[34]
Medication deactivation packets were purchased and distributed to the public to facilitate proper disposal.[35] In addition, these packets were provided to rural physician practices, pharmacies, and hospice facilities throughout the State.[36] One municipality in the State also requested packets for residents of the town as part of a community outreach project. Requests were made of stakeholders to secure permanent drop boxes, as well as to host take-back days in partnership with state law enforcement and representatives from the state Drug Enforcement Administration (DEA) office.[37] Funding and support was provided through the Project, depending on the needs of the stakeholders.
Overall, the Project met several of its objectives. By utilizing the information provided in the SCRIPTS program—as well as guidelines set forth by federal and state agencies—the grant was able to demonstrate positive effects on safe prescribing and education on the appropriate use and disposal of opioids. The number of opioid prescriptions dispensed per month declined since the Project was implemented,[38] and the number of prescriptions for medications for opioid withdrawal increased overall since 2015.[39] Additionally, the amount of disposed medications and number of sites participating in take-back programs increased over the life of the Project.[40] Data of deaths due to opioid use beyond 2016 has not been published yet; therefore, specific evaluation of this outcome is not included in this Article. Outcomes and results due to specific aspects of the Project are further discussed below and are presented in figures 2, 3, and 4.
A total of six pharmacists were recruited, trained, and served as detailers during this project. Approximately twenty provider, dispenser, and patient group presentations were given, and over fifty academic detailing site visits were conducted. More than one thousand toolkits were distributed during the presentations and site visits, as well as at substance abuse-focused conferences across the State. Since the start of the academic detailing portion of the Project in 2017, the number of enrollees in SCRIPTS increased from 5,195 in January 2016 to 19,909 as of October 2017.[41] The number of unique inquiries also increased over the duration of the Project.[42]
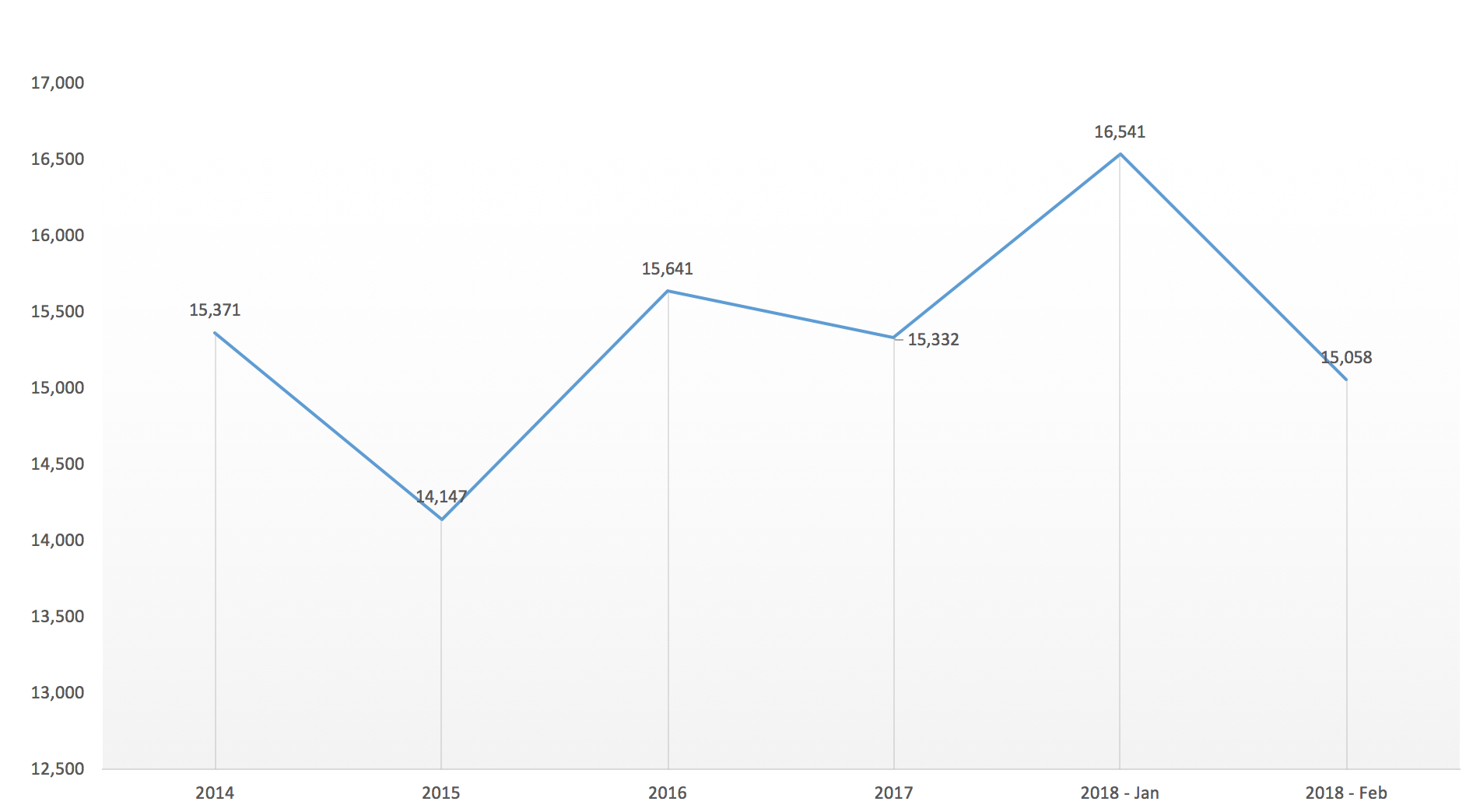
Another aspect of the academic detailing program provided evidence-based recommendations for chronic pain management, with the intent to decrease the inappropriate prescribing or utilization of opioids.[43] The average number of opioid prescriptions dispensed monthly in the State has steadily declined since 2015 to a low of approximately 75,000 in February 2018.[44] The number of prescriptions dispensed for opioid withdrawal treatments peaked at 16,541 prescriptions in January 2018, compared to 14,147 prescriptions in 2015 prior to the start of the grant project.[45] Opioid withdrawal treatments included buprenorphine and naltrexone prescriptions only.
Radio ads were broadcast on forty-seven separate radio stations in three radio regions—including major metropolitan and surrounding areas—over a six-month time period.[46] Over nineteen thousand ads were run each month during this time period, reaching approximately 1.2 million people.[47] Analyses of the social media and online programs demonstrated an average of twelve thousand views of posted videos, over fourteen thousand visits to the website, and an estimated one-million people reached per month.[48]
Participation in medication disposal increased over the duration of the Project. Specifically, the number of counties participating in take-back events or housing permanent drop box locations increased from nineteen counties in 2015 to twenty-nine (out of forty-six total) by the end of 2017.[49] The actual number of permanent drop box sites increased from thirty-two to one hundred over the same time period.[50] The amount of disposed medications at DEA-sponsored events increased steadily throughout the Project from 6,688 pounds in April 2016 to 9,032 pounds in October 2017.[51] Fifteen counties are still without a permanent drop box or take-back site,[52] however they were contacted about the availability of medication deactivation packets. These packets will continue to be distributed throughout the State upon request. Approximately 2,800 deactivation packets have been distributed to date.[53]
Through partnerships with law enforcement, state agencies, and pharmacy leadership, the initiatives in the preSCriptions Medication Safety Matters project contributed to a reduction in opioid prescribing and increased public awareness of the opioid crisis in the State. Data from the SCRIPTS enrollment and inquiries for the first quarter of 2018 was not available at the time of manuscript creation. However, it is likely that the number of enrollees and unique inquiries has steadily increased.
There are several limitations that must be discussed with this Project. As the attention to the opioid crisis in the State increased, initiatives and efforts to reduce the problem also increased. In May 2017, the Governor of South Carolina signed H 3824 into law, mandating that all prescribers of Schedule II Controlled Substances check the Prescription Monitoring Program prior to prescribing.[54] This likely accounted for some increase in the number of enrollees as well as unique inquiries.[55] In addition, there was an increase in enrollees and inquiries prior to enacting this particular legislation. In April 2016, the South Carolina Department of Health and Human Services—the State’s administrator of Medicaid services and benefits—required verification of Medicaid members’ controlled substance history in SCRIPTS prior to prescribing opioid medications.[56] Also, the integration of the Prescription Monitoring Program into the electronic health records of several large health-systems occurred, which may have streamlined access and increased SCRIPTS monitoring. However, the academic detailers were still able to provide best practice advice and guidance for prescribers unfamiliar with the Prescription Monitoring Program.
The number of academic detailing services was limited due to time constraints. The academic detailing service began in year two of the grant project, as the first year focused on development of materials and recruitment of detailers. Training of detailers was conducted once materials were printed and ready for distribution, which delayed the start of this service. In addition, all detailers participating in the Project were only available on a part-time basis due to being full-time employees with other entities or organizations.
Availability of data and statistics regarding other goals was limited. Enrollment in substance use disorder treatment programs is reported to the Substance Abuse and Mental Health Services Administration (SAMHSA) annually, and it is at least one to two years behind current trends.[57] Likewise, statistics related to emergency room visits and overdose deaths are approximately two years behind.[58] These goals will continue to be tracked over time to fully understand the impact of this project.
Based upon the success of this program in several areas, there are many opportunities to expand efforts. While primary care providers were mostly targeted through the grant for academic detailing services, other providers may also benefit from educational visits. These potential beneficiaries include emergency department and urgent care prescribers, hospitalists or other acute care providers, and orthopedic specialists. These groups may initiate therapies for opioids when other alternatives may be available. Patients seeking opioid prescriptions may also present to these providers—especially the emergency department—so targeted education on evidence-based methods to optimize the use of appropriate treatment regimens for chronic pain while limiting opioid medications may be beneficial.
The program identified a need in rural areas—due to a high patient-to-provider ratio—compared with the urban areas.[59] Academic detailing services and educational programming—specifically in rural practices—may help to reduce the number of prescriptions of chronic pain medications in these areas. Pharmacists in these rural areas should also be included in academic detailing services and programming, as they are likely facing similar issues on a daily basis. Specific education about prescribing and dispensing naloxone—particularly in rural areas—is needed so that patients have access to potentially life-saving medications. To further reduce opioid misuse, collaboration between prescribers and local pharmacists is also encouraged.
The rise of opioid misuse and related deaths prompted the preSCriptions Medication Safety Matters project in South Carolina. Due to the many factors that are associated with this issue, a multi-faceted approach was utilized. Several interventions that targeted prescribers, dispensers, and the public were implemented across the State in collaboration with several stakeholders, including state agencies, pharmacies, and academics. These interventions have led to reduced prescriptions of opioid medications and increased utilizations of the State’s Prescription Monitoring Program.[60] Many opportunities exist to expand these efforts by building upon the momentum generated by this project.
Figure 1. Sample tool used for detailing prescribers
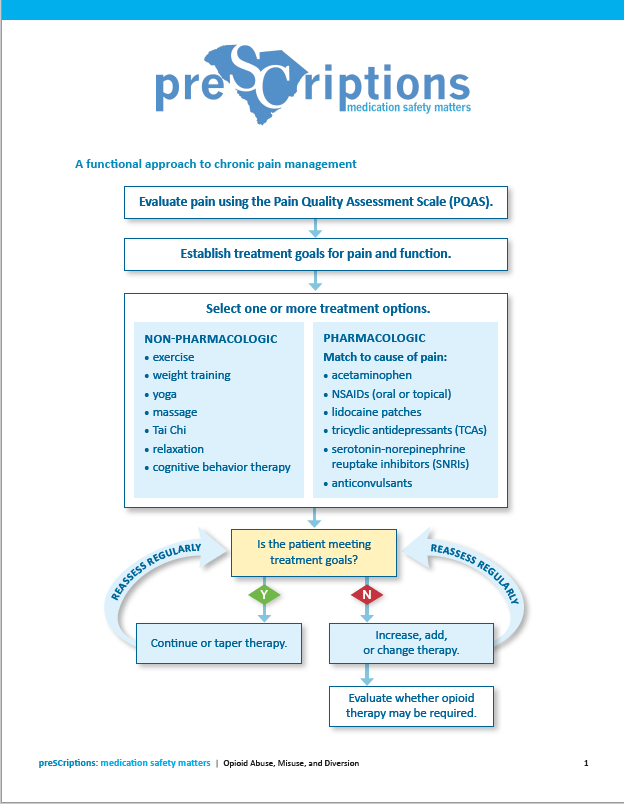
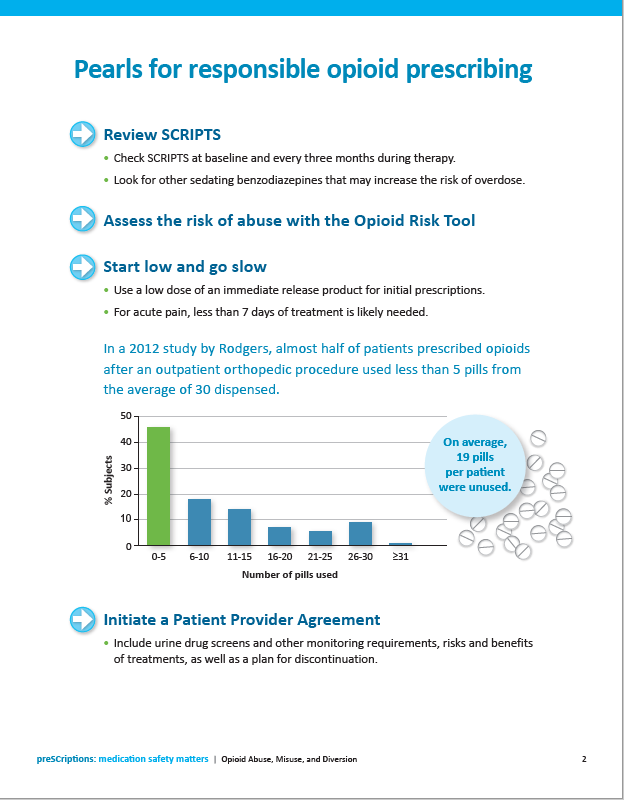
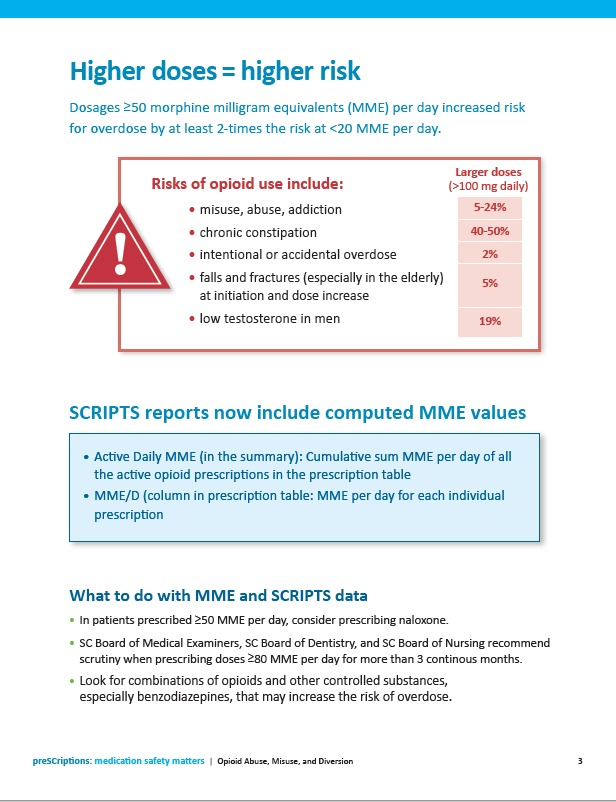
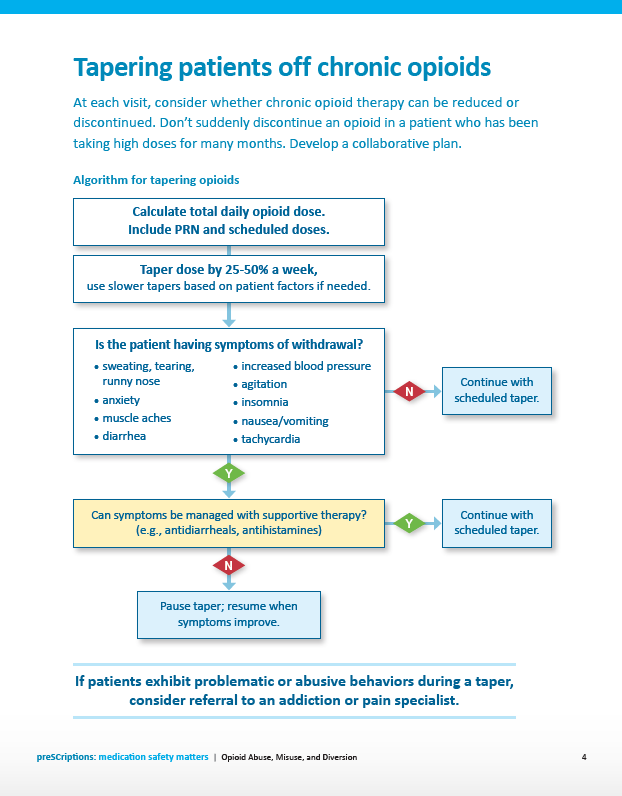
Figure 2. SCRIPTS Enrollees from January 2016 (prior to project) through October 2017
Figure 3. Unique Inquiries in SCRIPTS
Figure 4. Average number of opioid withdrawal prescriptions dispensed monthly in South Carolina